Lifestyle and mental health in preschool- and primary school-aged children
While mental health disorders are much less common in preschool- and primary-school-aged children than in adolescents or adults, many problems that arise in later years are rooted in the earlier stages of life (Jones 2013). Like physical health, mental health is influenced by genetic factors, but the physical and psychosocial environment surrounding the child also plays an important role, along with the related lifestyle, including eating and physical activity habits and sleep patterns. One of the factors
that might affect mental health the most is adverse childhood experiences, such as abuse and violence, parental divorce or the death of a family member, and other stressful life events (Shonkoff and Garner 2012). Strong, repeated or prolonged stress has a negative impact on the child’s neurological development. This can cause problems with learning ability, memory and behaviour or lead to mental health disorders (Shonkoff and Garner 2012). The importance of lifestyle for mental health is difficult to assess because the associations between lifestyle and mental health are reciprocal, and both also depend on other factors, such as socioeconomic status. Since lifestyle is something people can change and unhealthy habits affect many people, lifestyle deserves continued attention in promoting mental health.
This is especially the case with children because the lifestyle adopted at a young age is often followed into adulthood, so positive or negative habits taken up early in life can have a lifelong effect on mental health.
This article outlines the mental well-being of Estonian children aged 2 to 10 years and describes its associations with socioeconomic characteristics and health-related behaviour to highlight potential factors contributing to inequality. Research on the mental health and well-being of preschool- and primary-school-aged children is scarce, especially on the youngest children, compared to other age groups. This is due to the fact that conducting such research is expensive and methodologically complex. Young children often lack the capacity to clearly communicate their mental state, and because of this, researchers often have to rely on assessments from bystanders, such as parents or teachers. However, their assessments may not always be accurate or reflect the child’s subjective experience. In Estonia, as elsewhere, there are currently few large-scale studies available that provide an overview of the mental well-being of preschool- and primary-school-age children and compare it with lifestyle.
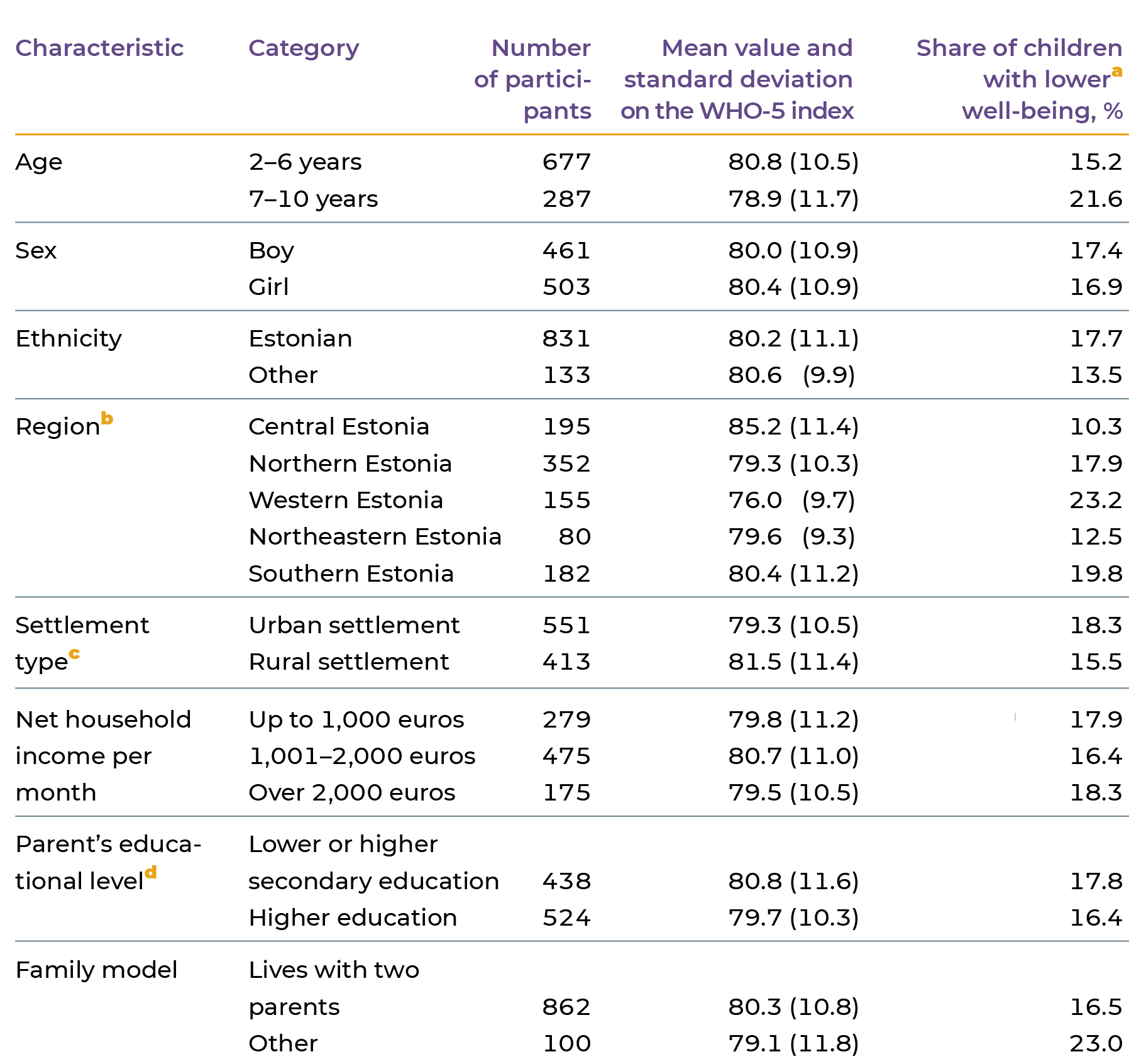
This article is primarily based on the data collected in the course of the 2013–2015 Estonian National Dietary Survey. The strength of this survey is that it can provide detailed and versatile data on the subject of children’s lifestyle that is representative of the population. As a cross-sectional study, it does not allow for the identification of causal associations, but the results nevertheless help pinpoint potential issues. Thanks to its representative sample, the study also offers a more comprehensive overview of the mental health situation of Estonian children than, for example, the insight gained form vulnerable groups. The methodology report describes how the study was conducted (Nurk et al. 2017). Data was collected on nearly 1,000 children aged 2 to 10 years by interviewing their parents or guardians. About 30% of the children were aged between 7 and 10 years, and more than 90% of these children went to school (tabel 2.1.1). By contrast, there were hardly any school children between the ages of 2 to 6. The sample included a more or less equal number of boys and girls, and 85% of the children were from families with an Estonian background. The WHO-5 Well-Being Index developed by the World Health Organisation (WHO) was used in the study to assess children’s mental health.
THE WHO-5 WELL-BEING INDEX MEASURES THE LEVEL OF SUBJECTIVE WELL-BEING
The well-being index developed by the World Health Organisation (The 5-item WHO Well-Being Index – WHO-5) assesses the respondent’s psychological well-being during the previous two weeks (Topp et al. 2015). The WHO-5 questionnaireconsists of five statements (how often the respondent has felt cheerful and in good spirits; calm and relaxed; active and vigorous; fresh and rested; engaged in things that interested them). Respondents rate these on a scale from 0 (at no time) to 5 (all the time). To calculate the index, the responses are summed and multiplied by four in order to express well-being on a simplified scale from 0 (absence of well-being) to 100 (the greatest possible well-being). Using data from the Estonian National Dietary Survey, the analysis section of this article compares children with lower well-being with children with higher well-being. Since the WHO-5 index does not specify a universally recognised meaningful cutoff point in the age group of children between 2 and 10 years of age, the authors of the article have designated one-fifth of the children who scored at the lower end of the scale as the group with lower well-being. More specifically, children with a WHO-5 score value of < 72 were selected as the group with lower well-being.
While the mental health of Estonian children can be described as good, well-being decreases with age
Based on the Estonian National Dietary Survey, the WHO-5 index in children aged between 2 and 10 years varied between 44–100; the average score was 80. The average score was 81 for 2-to-6-year-olds and 79 for 6-to-10-year-olds (tabel 2.1.1). While the WHO-5 index has not previously been used to assess children between the ages of 2 and 8, the measurement scale has been validated for screening depression in children aged between 9 and 12, with a total score value of 40 deemed an appropriate cutoff (Allgaier et al. 2012).
None of the children in the dietary survey scored this low. In the European Quality of Life Survey, the average score of the adult population of nearly 30 countries varied between 54 and 70 (Topp et al. 2015). Although the comparison with adults is not appropriate, it does suggest that according to the parents, the well-being of the children included in the study was quite high. It is worth bearing in mind that parents are not necessarily objective assessors – they know only what their child is like at home and not what they are like in kindergarten or school. Parents also tend to interpret their child’s mental state in a more positive light. Since young children are unable to communicate problems associated with their mental well-being, there is still no good alternative to indirect assessment. Here, involving different types of assessors – for example, teachers as well as parents – might help put together a more complete picture (Streimann et al. 2021).
Data from the Estonian National Dietary Survey can be compared with the results of the 2018 Children’s Worlds survey of children’s subjective well-being (Soo and Kutsar 2020). In all, 3,150 children aged 8, 10 and 12
years were interviewed for this study in Estonia. During the two weeks preceding the survey, 47% of 10-year-olds and 41% of 12-year-olds felt overwhelmingly positive emotions, i.e. they rated their level of emotional well-being as high. Most of the remaining 10-year-olds were cheerful and energetic, only occasionally feeling tense (25%), or alternated between positive and negative emotions (28%). Only a handful of children felt predominantly negative emotions. The mental well-being of children up to 10 years of age can therefore be rated as rather high, based on the children’s subjective experience. However, the share of low-spirited and apathetic children was significantly higher (15%) among 12-year-olds. The general satisfaction with life also decreased with age: three-quarters of the 8- and 10-year-olds gave the highest satisfaction rating, while only about half of the 12-year-olds were perfectly satisfied with their life.
Children’s mental well-being likewise declined with age in the Estonian National Dietary Survey. In the survey, a model adjusted for all socioeconomic characteristics showed that, compared to children aged 2 to 6 years, children aged 7 to 10 years had 1.5 times the odds of having lower well-being (Figure 2.1.1). The sharp increase in problems during adolescence may partly be due to the use of indirect assessors for young children. However, since the subjective assessments of both parents and children point to a similar conclusion, the deterioration of children’s mental health as they get older still seems to be a real tendency and not just a product of methodology.
According to data from the Estonian National Dietary Survey, well-being varied little between boys and girls, or between Estonian children and those of other ethnicities. Furthermore, well-being was not associated with the settlement type, family income, parent’s educational level or family model (Figure 2.1.1), which indicates a low level of socioeconomic inequality.
However, mental wellbeing was significantly associated with the region of residence, with children from central Estonia standing out with the highest wellbeing (Table 2.1.1 and Figure 2.1.1). Compared to children from central Estonia, children from northern, southern and western Estonia had 2.2–2.6 times higher odds of having lower wellbeing.
The study of children’s subjective well-being (Soo and Kutsar 2020) also examined how the children’s well-being assessment related to their social environment and family model. Children who felt overwhelmingly positive emotions and were completely satisfied with life rated their well-being at home, at school and in interactions with friends higher than others did. In addition, the results showed that 10- and 12-year-old children who lived with both biological parents had experienced more positive emotions during the previous two weeks (44%) than children who lived with a stepparent or a single parent (35%). This result differs from that of the Estonian National Dietary Survey, which found no association between well-being and family model. A possible explanation is that, as the Estonian National Dietary Survey did not differentiate between biological and stepparents, mental well-being may be primarily influenced by the quality of family relationships rather than any other benefits of growing up with two parents, such as economic security.
Notes:
a Children with a WHO-5 index score of < 72 make up the group with lower well-being.
b Northern Estonia: Harjumaa; western Estonia: Hiiumaa, Läänemaa, Pärnumaa and Saaremaa; central Estonia: Järvamaa, Lääne-Virumaa and Raplamaa; northeastern Estonia: Ida-Virumaa; and southern Estonia: Jõgevamaa, Põlvamaa, Tartumaa, Valgamaa, Viljandimaa and Võrumaa.
c Urban settlements are cities, towns and cities without municipal status; rural settlements are small towns and villages.
d c Parent’s level of education represents the education of the parent (or guardian) with the highest level of education living with the child.
J2.1.1.R
maiko.koort
2023-06-26
library(ggplot2)
library(tidyr)
library(scales)
#faili sisselugemine ja andmete formaadi korrigeerimine
J211=read.csv("PT2-T2.1-J2.1.1.csv",header=TRUE, encoding ="UTF-8")
names(J211)=J211[1,]
J211=J211[2:21,1:6]
tunnus=trimws(J211$Tunnus[c(1,3,5,7,12,14,17,19)])
J211=rbind(J211[c(2,4,6,8:11,13,15,16,18,20),])
J211$tunnusx=""
J211$tunnusx[1:3]=tunnus[1:3]
J211$tunnusx[4:7]=tunnus[4]
J211$tunnusx[8]=tunnus[5]
J211$tunnusx[9:10]=tunnus[6]
J211$tunnusx[11:12]=tunnus[7:8]
names(J211)[2]="OR"
J211$OR=as.numeric(J211$OR)
J211$LCI=as.numeric(J211$LCI)
J211$UCI=as.numeric(J211$UCI)
J211$tunnusx=as.factor(J211$tunnusx)
J211$tunnusx=factor(J211$tunnusx,levels=rev(levels(J211$tunnusx)[order(c(4,3,1,5,6,7,2,8))]))
#joonis
ggplot(J211)+
facet_grid(tunnusx~.,scales="free",space="free")+
geom_point(aes(x=Tunnus,y=OR,col=tunnusx),cex=3)+
geom_errorbar(aes(x=Tunnus,ymin=LCI,ymax=UCI,col=tunnusx),width=0.2,linewidth=1)+
geom_abline(slope=0,intercept=1,linewidth=0.1)+
theme_minimal()+
scale_color_manual(values=c("#668080", "#668080","#668080","#f09d00","#295200","#295200","#8fa300","#8fa300"))+
theme(text = element_text(color="#668080"),axis.text=element_text(color="#668080"))+
theme(legend.position = "none")+
coord_flip()+
xlab("")+
ylab("")+
theme(strip.text.y = element_text(angle = 360,face="bold",color="#668080"))
See footnotes in Table 2.1.1 for descriptions of the characteristics.
While the diet of Estonian pre-school- and primary-school-aged children features too few fruits and vegetables and too many sweets, mental well-being is not associated with diet
FOOD DIARIES HELP GAIN INSIGHT INTO THE HEALTHINESS OF EATING HABITS
The parents of the children participating in the Estonian National Dietary Survey recorded the quantity of all the foods and drinks consumed by the child during the two days of the survey. The resulting food diaries were used to calculate how many grams of fruits and vegetables and high-calorie, nutrient-poor foods (sweets, sweet and savoury snacks, ice cream, sweet bakery and pastry products, etc.) the child ate during the day. The gram amounts were then converted into numbers of servings based on specific caloric value assigned to food groups. Eating fruits and vegetables is typically associated with healthy eating habits, and consuming high-calorie, nutrient-poor foods indicates less favourable eating habits; however, the authors additionally calculated a diet quality index to describe the healthfulness of the overall diet. To calculate the index, it was assessed how well the respondent’s diet accords with the Estonian dietary recommendations, taking into account food groups and the availability of nutrients. Food group and nutrient scores were then summed and expressed on a scale of 0 (complete lack of accordance) to 100 (complete accordance).
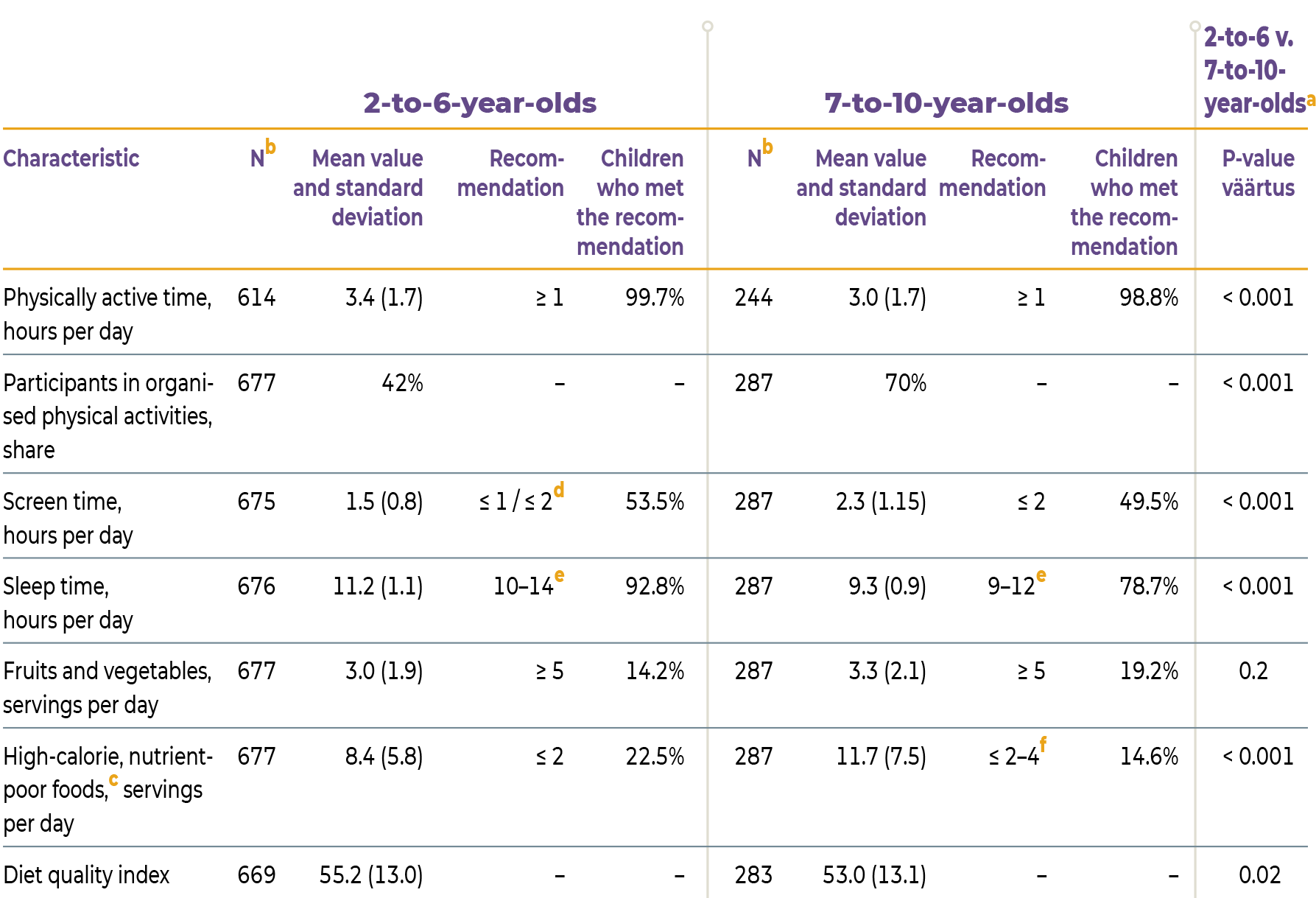
Based on the National Dietary Survey, the eating habits of Estonian children from 2 to 10 years of age leave much to be desired. In contrast to dietary recommendations which call for at least five servings of fruits and vegetables per day, the children who participated in the survey consumed an average of only three servings per day, with only 14% of children aged 2 to 6 and 19% of children aged 7 to 10 eating recommended amounts (Table 2.1.2). Depending on the child’s age and energy needs, they should have no more than 2 to 4 servings of sweets and snacks each day. Yet children aged 2 to 6 years consumed an average of eight servings and children aged 7 to 10 years an average of 12 servings of these foods a day. Twenty-two percent of the younger children and 15% of the older children met the dietary recommendation for high-calorie, nutrient-poor foods. The age difference was also expressed in the nutrition quality index, which was somewhat higher for the younger age group than it was for the 7-to-10-year-olds. The eating habits of older children probably deteriorate as they become more independent in determining their food choices.
The associations between nutrition and mental health can be studied in a number of ways, but the pattern emerging from various studies is that children with healthier eating habits usually also have better mental health indicators (Khalid et al. 2017). Like other organs, the brain also relies on nutrients for its development and functions, so it is highly likely that diet directly impacts mental health through physiological mechanisms (Lang et al. 2015). In real life, however, physiological mechanisms are only one way in which mental health is associated with nutrition. Both diet and mental health, in turn, depend on socioeconomic factors, and mealtimes also affect mental well-being as time spent together as a family. In addition, the effects of diet and mental health are likely reciprocal – an unhealthy menu can also be a result of mental health issues, not necessarily the other way around. Therefore, the associations between nutrition and mental health may not always be obvious. The National Dietary Survey also failed to reveal any significant correlation between children’s mental well-being and their diet (Figure 2.1.2).
Physical activity has a positive association with mental well-being while passive screen time has a negative one
Along with nutrition, physical activity habits are an important factor affecting both physical and mental health in many ways throughout the life course.
On the one hand, physical activity habits are characterised by any form of movement that consumes energy, whether related to training, entertainment, work or getting from one place to another. On the other hand, physical activity habits are characterised by sedentary lifestyle activities, including physically inactive screen time with a TV, computer or smart device. Similar to nutrition, physical activity is likely associated with mental health through several factors, including both neurological and psychosocial mechanisms (Lubans et al. 2016). In children and adolescents, much like in adults, physical activity is associated with better mental health and passive screen time with poorer mental health, although the associations between physical activity habits and mental health are more evident in adolescents than in children, and there has been very little research on the topic, especially in preschool-aged children (Rodriguez‑Ayllon et al. 2019).
On average, children aged 2 to 6 years who took part in the National Dietary Survey were physically active for more than three hours a day, while children aged 7 to 10 years were physically active for almost three hours a day (Table 2.1.2). In light of the WHO recommendation for children to spend at least one hour a day being physically active, almost all children included in the analyses got enough active time. Meanwhile, less than half of 2-to-6-year-olds and 70% of 7-to-10-year-olds participated in organised sports or other physical activities. Children’s mental well-being was significantly associated with physically active time: for every hour added to daily physical activity, the odds for lower well-being decreased by 19% (Figure 2.1.2). Whether the active time included participation in organised activities made no difference.
In order to provide parents with instructions for guiding children’s health behaviour, Estonian nutrition and exercise recommendations, suggest that the screen time of 2-to-4-year-olds should not exceed one hour a day, while that of 5-to-17-year-olds should be limited to two hours a day. Screen time remained within the recommended limits for about half of both 2-to-6-year-olds and 7-to-10-year-olds. The association between screen time and children’s mental well-being was significant, with every hour added to daily screen time increasing the odds of lower well-being by 1.26 times (i.e. a 26% increase). The association between screen time and mental health is not necessarily due to a lack of physical activity alone. Exposure to inappropriate media content can also leave its mark, as well as the fact that excessive screen time tends to reduce both the duration and quality of children’s sleep. The broader meaning of the usage patterns of digital devices from the perspective of mental well-being is discussed in Chapter 4 (‘Digital technologies and mental well-being’).
Children up to 6 years of age generally get enough sleep, but the amount of sleep tends to decrease as children age, possibly increasing the role of sleep in mental health
Among the participants of the National Dietary Survey, children aged 2 to 6 years slept an average of 11 hours a day, while children aged 7 to 10 years slept an average of 9 hours a day. While no national health behaviour recommendations concerning the duration of children’s sleep have been published in Estonia, according to the recommendations issued in several other countries, including, for example, recommendations in the United States, children aged 1 to 2 years should get 11–14 hours of sleep, children aged 3 to 5 years should get 10–13 hours of sleep and children aged 6 to 12 years should get 9–12 hours of sleep every day. In the National Dietary Survey, 93% of preschoolers and 78% of school-aged children got a daily amount of sleep in line with this recommendation, and no significant associations between sleep time and mental well-being were detected. The study of children’s subjective well-being (Soo et al. Kutsar 2020) also looked into the duration of children’s nighttime sleep.
Fifty-five percent of children who felt predominantly negative emotions slept for less than eight hours. Although the dietary survey did not find an association between sleep and mental health, the results did suggest that sleep deficit becomes a more significant factor after children reach school age. A likely explanation is that the younger the child is, the more control parents have over their behaviour. Different research conclusions about the importance of night-time sleep may partly be due to the use of different indicators for mental well-being. At any rate, the importance of sleep for mental health seems to become more definite as the child grows more independent.
Notes:
aFor organised physical activities, the difference between age groups was tested using logistic regression, while all other characteristics were tested using analysis of variance.
b No more than one hour per day for children aged up to 5, no more than two hours per day for children aged 5 and up
c According to age: 11–14 hours for 1-to-2-year-olds, 10–13 hours for 3-to-5-year-olds and 9–12 hours for 6-to-12-year-olds.
d According to age, sex and energy requirements:≤ 2 servings for 7-to-8-year-olds, ≤ 3 servings for 8-to-9-year-olds and ≤ 4 servings for 9-to-10-year-olds. One serving is approximately 40 kcal.
e Sweets, sweet and savoury snacks, ice cream, sweet bakery and pastry products, etc.
J2.1.2.R
maiko.koort
2023-06-26
library(ggplot2)
library(tidyr)
library(scales)
library(dplyr)##
## Attaching package: 'dplyr'## The following objects are masked from 'package:stats':
##
## filter, lag## The following objects are masked from 'package:base':
##
## intersect, setdiff, setequal, union#faili sisselugemine ja andmete formaadi korrigeerimine
J212=na.omit(read.csv("PT2-T2.1-J2.1.2.csv",header=TRUE, encoding ="UTF-8"))
names(J212)[2]="OR"
J212$OR=as.numeric(J212$OR)
J212$Tunnus=as.factor(J212$Tunnus)
J212$Tunnus=factor(J212$Tunnus,levels(J212$Tunnus)[order(c(5,2,7,6,3,1,4))])
#joonis
ggplot(J212,aes(x=Tunnus,y=OR))+
geom_point(aes(col=Tunnus),size=3,show.legend=FALSE)+
geom_errorbar(aes(x=Tunnus,ymin=LCI,ymax=UCI,col=Tunnus),width=0.1,linewidth=0.9,show.legend=FALSE)+
theme_minimal()+
scale_color_manual(values=c("#1E272E","#1E272E","#1E272E","#1E272E","#FF3600","#1E272E","#8fa300"))+
theme(text = element_text(color="#668080"),axis.text=element_text(color="#668080"))+
coord_flip()+
xlab("")+
geom_abline(aes(slope=0,intercept=1),linewidth=0.4,col="#f09d00")+
ylab("")
Note: The associations between each characteristic and mental well-being (lower v. higher) were tested using logistic regression analysis. The models are adjusted for the socioeconomic background of the child (age, sex, ethnicity, region of residence, type of settlement, family income, parent’s level of education and family model). A higher odds ratio indicates greater odds of experiencing lower well-being (WHO-5 index value < 72).
Source: figure by the authors, based on data from the 2013–2015 Estonian National Dietary Survey
Summary
Population-based data show that parents rate the mental well-being of Estonian children aged 2 to 10 years as relatively good. However, it is worth remembering that well-being assessments are mostly biased in a more positive direction.
The association between mental health and lifestyle is not that pronounced at preschool and primary-school age, as mental well-being varies little across socioeconomic characteristics and lifestyle. An unbalanced diet is reflected as a negative aspect in children’s lifestyle: children eat too few fruits and vegetables and too many sweets. While Estonian children between the ages of 2 and 10 years spend enough time being physically active and children between the ages of 2 and 6 years get enough sleep, a fifth of school-age children tend to sleep too little. Regardless of age, however, roughly half of children spend too much time looking at screens. The strongest association between mental health and lifestyle in Estonian children emerged with physical activity: there was a positive association with physical activity and a negative association with passive screen time.
Allgaier, A.-K., Pietsch, K., Frühe, B., Prast, E., Sigl-Glöckner, J., Schulte-Körne, G. (2012). Depression in pediatric care: is the WHO-Five Well-Being Index a valid screening instrument for children and adolescents? General Hospital Psychiatry 3, 234-241. https://doi.org/10.1016/j.genhosppsych.2012.01.007
Jones, P. B. (2013). Adult mental health disorders and their age at onset. The British Journal of Psychiatry 202, s5–s10. https://doi.org/10.1192/bjp.bp.112.119164
Khalid, S., Williams, C. M., Reynolds, S. A. (2017). Is there an association between diet and depression in children and adolescents? A systematic review. British Journal of Nutrition 116, 2097–2108. https://doi.org/10.1017/S0007114516004359
Lang, U. E., Beglinger, C., Schweinfurth, N., Walter, M., Borgwardt, S. (2015). Nutritional aspects of depression. Cellular Physiology and Biochemistry 37, 1029–1043. https://doi.org/10.1159/000430229
Lubans, D., Richards, J., Hillman, C., Faulkner, G., Beauchamp, M., Nilsson, M., Kelly, P., Smith, J., Raine, L., Biddle, S. (2016). Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics 138, e20161642. https://doi.org/10.1542/peds.2016-1642
Nurk, E., Nelis, K., Saamel, M., Martverk, M., Jõeleht, A., Nelis, L. (2017). National Dietary Survey among children up to ten years old and breastfeeding mothers in Estonia. EFSA Supporting Publications 14, EN-1199. https://doi.org/10.2903/sp.efsa.2017.EN-1199
Rodriguez‑Ayllon, M., Cadenas‑Sánchez, C., Estévez‑López, F., Muñoz, N. E., Mora‑Gonzalez, J., Migueles, J. H., Molina‑García, P., Henriksson, H., Mena‑Molina, A., Martínez‑Vizcaíno, V., Catena, A., Löf, M., Erickson, K. I., Lubans, D. R., Ortega, F. B., Esteban‑Cornejo, I. (2019). Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta‑analysis. Sports Medicine 49:1383–1410. https://doi.org/10.1007/s40279-019-01099-5
Shonkoff, J. P., Garner, A. S. (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics 129, e232-e246. https://doi.org/10.1542/peds.2011-2663
Soo, K., Kutsar, D. (2020). Kuidas elad, Eestimaa laps? Ülevaade 8–12-aastaste laste subjektiivsest heaolust. Tartu ülikooli ühiskonnateaduste instituut. https://isciweb.org/wp-content/uploads/2020/04/%D7%9C%D7%94%D7%A2%D7%9C%D7%95%D7%AA-%D7%90%D7%97%D7%A8%D7%99-8-%D7%91%D7%90%D7%A4%D7%A8%D7%99%D7%9CHow-are-the-Estonian-Children.pdf
Streimann, K., Sisask, M., Toros, K. (2021). Children’s mental health in different contexts: Results from a multi-informant assessment of Estonian first-grade students. School Psychology International 42, 379–397. https://doi.org/10.1177/01430343211000414
Topp, C. W., Østergaard, S. D., Søndergaard, S., Becha, P. (2015). The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychotherapy and Psychosomatics 84, 167–176. https://doi.org/10.1159/000376585