Young people’s mental health and well-being and its relationship with lifestyle
Young people’s well-being and health behaviour are largely influenced by their parents’ beliefs and health behaviour. Many lifestyle factors support mental well-being, such as a healthy diet, sufficient sleep and physical activity. On the other hand, adolescent independence often comes with a craving for new experiences and the desire to test boundaries, which can involve experimentation with drugs. This can, in turn, affect young people’s mental well-being. Adolescence impacts people’s ability to cope with their emotions, and one solution may be to seek relief from using psychoactive substances. The first substances young people most often come into contact with are tobacco and alcohol, but also cannabis and stimulants or sedatives/hypnotics used for non-medical purposes (ESPAD report 2019).
This article provides an overview of Estonian adolescents’ mental health and well-being over the last two decades and their relationship with lifestyle and socioeconomic factors.
Current research increasingly treats mental health outside the framework of psychiatric illness, with a clear focus on psychosocial well-being (Moore et al. 2019). Many factors influence psychosocial well-being during childhood and adolescence. This is the inception period for several behavioural risk factors that can contribute to lifestyle-related disease. These factors include an unhealthy diet, physical inactivity, smoking and alcohol consumption, which can result in habits that carry over into adulthood. The 21st century has brought dramatic changes in the everyday life of young people, including their health behaviour. These have transformed, for example, the nutritional composition of food and eating habits more generally, decreased physical skills and activity, as well as increased the selection and availability of drugs.
Adolescent health and well-being are influenced by a number of individual, behavioural, social, cultural, environmental and organisational factors that operate on different levels and change over time (Inchley et al. 2020). This calls for updated risk models that involve youth behaviour and related factors and reflect the social context. The social context combines the immediate social environment that young people inhabit (e.g., family, peers and school) and broader social systems (e.g., education, healthcare, politics and the economy), while individual components include identity, attitudes, and biological aspects. The adolescent years provide an opportunity for prevention and intervention to support young people’s healthy development, promote physical as well as mental health and well-being in adulthood, and thereby improve the health of the next generation.
Our analysis is based on data from the study Health Behaviour in School-Aged Children, HBSC) andmed (Oja et al. 2019). HBSC is an international survey that has been conducted in Estonia since 1993. It has taken place every four years, for a total of eight times. The study provides a regular and comprehensive overview of the health status and well-being of adolescents aged 11, 13 and 15. It is the only population-based study on health behaviour with a representative sample of young people in Estonia. Our analysis relies on data from six waves of the study that span from 2002 to 2022 and feature the relevant characteristics associated with mental health. Each wave contains the health behaviour data of an average of 5,000 adolescents. The results are compared with neighbouring countries based on data from the 2018 survey.
In what follows, we use two variables to describe young people’s mental health: (1) sadness and depressive symptoms over the past six months and (2) periods of depressiveness lasting two weeks or longer over the past 12 months. While the absence of these symptoms does not necessarily indicate high levels of mental well-being, measurable characteristics make it possible to assess young people’s mental health. The survey has inquired about sadness and depressive symptoms in all participating countries since 2002, which enables Estonian data to be compared with data from other countries. Questions about a two-week period of depressiveness have been featured in the survey since 2006. The comparison period is therefore shorter, and since not all countries have included this question in the survey, this data cannot be used in international comparisons. However, because a period of depressiveness lasting for two weeks or longer indicates a more serious mental health problem, we took this variable as the basis for assessing the relationship between mental health and socioeconomic and lifestyle factors.
During the reference period of 2002–2022, the prevalence of sadness and depressive symptoms in Estonian adolescents was lowest in 2006 and 2010. In those years, less than a quarter of girls and a tenth of boys experienced these feelings more than once a week in the previous six months (Figure 2.2.1). The prevalence of depressive symptoms was the highest for girls in 2022 and for boys in 2002.
Based on data from the latest survey, as many as 40% of girls and nearly 20% of boys felt sad or depressed more than once a week during the previous six months.
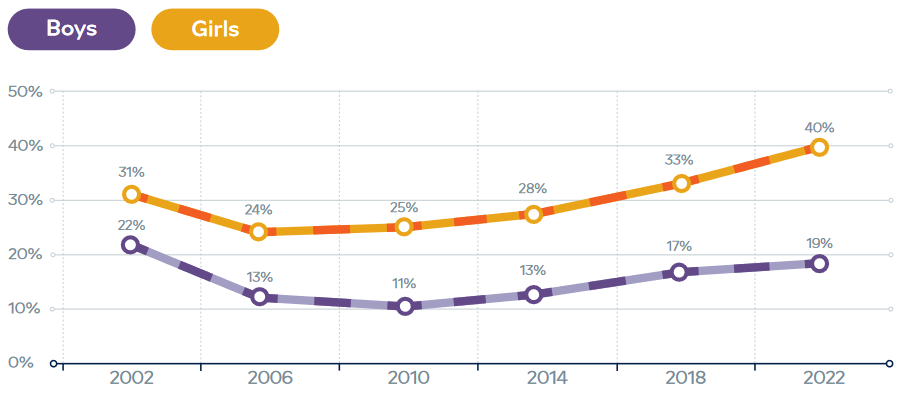
Figure 2.2.2 describes the experience of a period of depressiveness lasting for two weeks or longer during the previous year, for the period of 2006–2022. As with the previous figure, it shows that periods of depressiveness were more frequent in girls than in boys and that there has been an increase in the trend since 2010, regardless of gender. It is difficult to say whether this increase is related to young people perceiving their lives as more problematic or whether they are simply more aware of and attentive to their feelings.
J2.2.2.R
maiko.koort
2023-06-27
library(ggplot2)
library(tidyr)
library(scales)
#faili sisselugemine ja andmete formaadi korrigeerimine
J222=read.csv("PT2-T2.2-J2.2.2.csv",header=TRUE, encoding ="UTF-8")
J222=pivot_longer(J222,c("Boys","Girls"))
names(J222)=c("Year","Gender","Protsent")
J222$Year=as.factor(J222$Year)
#joonis
ggplot(J222,aes(x=Year,y=Protsent,col=Gender))+
geom_point(cex=3)+
geom_line(aes(col=Gender,group=Gender),linewidth=1)+
theme_minimal()+
theme(legend.position = "bottom")+
ylab("Share of young people (%)")+
scale_y_continuous(limits=c(0,50))+
scale_color_manual(values=c("#6666cc","#FF3600"))+
theme(text = element_text(color="#668080"),axis.text=element_text(color="#668080"))
Comparing Estonian adolescents with their peers in neighbouring countries revealed that in all the analysed age groups, there were significantly more girls and boys in Estonia who have felt sad and depressed more than once a week than there were in Latvia, Lithuania, Finland or Sweden (Figure 2.2.3). In addition, Estonian scores were significantly higher than the average of the 45 countries participating in the HBSC survey.
Nevertheless, comparing data from 2018 with those from the previous survey in 2014 revealed that the prevalence of sadness and depressive symptoms among 11-to-15-year-olds has increased in all the countries presented in the figure, regardless of age group and gender (Oja et al. 2019). The figure also shows that the occurrence of sadness and depressive symptoms increased with age; among girls, it almost doubled between the ages of 11 and 15.
J2.2.3.R
maiko.koort
2023-06-27
library(ggplot2)
library(tidyr)
library(scales)
#faili sisselugemine ja andmete formaadi korrigeerimine
J223=read.csv("PT2-T2.2-J2.2.3.csv",header=TRUE, encoding ="UTF-8")
J223=J223[1:7]
names(J223)[c(3,4)]="Boys"
names(J223)[c(6,7)]="Girls"
names(J223)=paste(names(J223),J223[1,])
J223=J223[2:7,]
J223=pivot_longer(J223,2:7)
J223=separate(J223,2,c("Sugu","Age")," ")
names(J223)[1]="Riik"
J223$value=as.numeric(J223$value)
J223x=subset(J223,Riik!="HBSC total")
J223y=subset(J223,Riik=="HBSC total")
#joonis
ggplot()+
facet_grid(~Sugu)+
geom_col(data=J223x,aes(x=Age,y=value,fill=Riik),pos=position_dodge(0.6),width=0.7)+
geom_line(data=J223y,aes(x=Age,y=value,group=Sugu,col=Riik),linewidth=1)+
geom_point(data=J223y,aes(x=Age,y=value,group=Sugu,col=Riik),cex=1.5)+
geom_text(data=J223y,aes(x=Age,y=value+2,group=Sugu,label=value),fontface="bold",cex=3,col="#FF3600")+
theme_minimal()+
theme(legend.position = "bottom",legend.title=element_blank())+
ylab("Share of young people (%)")+
scale_y_continuous(limits=c(0,50))+
scale_color_manual(values="#FF3600")+
scale_fill_manual(values=c("#f09d00","#bf6900","#6666cc","#4026cc","#668080"))+
theme(text = element_text(color="#668080"),axis.text=element_text(color="#668080"))+
theme(strip.text.x = element_text(face = "bold",size=10,color="#668080"))
Our primary social context is shaped by the family, which is the main source of lifestyle-related behavioural patterns. Studies show that nearly half of the mental health problems arising in adult years first appear during early adolescence and that neuropsychiatric disorders represent the main burden of disease among adolescents in wealthier countries (Kessler et al. 2007). The lower incidence of neuropsychiatric issues in poorer countries may partly be due to their lower standard of living, which makes problems related to meeting basic needs a priority over mental health problems, and results in the limited availability of psychological and psychiatric help. At the same time, early intervention is critical, especially with young people – the earlier the intervention, the more effective the solution. This is the case both in terms of the duration and intensity of the disorder and the occurrence of accompanying mental health problems (Kessler et al. 2007).
By analysing the relationship between mental health and socioeconomic factors in the case of Estonian adolescents, we found that depressiveness was significantly more common among young people with a home language other than Estonian and those in a poorer economic situation (Figure 2.2.4). In addition, the figure shows that girls and older age groups experienced depressiveness more frequently, which is in line with the findings expressed in previous figures.
J2.2.4.R
maiko.koort
2023-06-27
library(ggplot2)
#faili sisselugemine ja andmete formaadi korrigeerimine
J224=read.csv("PT2-T2.2-J2.2.4.csv",header=FALSE, encoding ="UTF-8")
J224$V1[2]="Sex"
J224$V1[4:5]="Age"
J224$V1[7]="Home language"
J224$V1[9:10]="Family’s economic situation"
J224$V1=as.factor(J224$V1)
J224$V1=factor(J224$V1,c("Sex","Age","Home language","Family’s economic situation"))
J224$V2=as.factor(J224$V2)
J224$V2=factor(J224$V2,levels(J224$V2)[order(c(1,2,3,4,7,5,6,8,9,10))])
#joonis
ggplot(J224)+
facet_grid(~V1,scales="free")+
geom_col(aes(x=V2,y=V3,fill=interaction(V1,V2,sep=":")),pos=position_dodge(0.6),width=0.8)+
geom_text(aes(x=V2,y=V3+1,group=V1,label=paste(V3,"%",sep="")),fontface="bold",cex=3.5,col="#668080")+
theme_minimal()+
scale_fill_manual(values=c("#6666cc","#6666cc","#6666cc","#f09d00","#668080","#668080","#668080","#bf6900","#4026cc","#FF3600"))+
theme(text = element_text(color="#668080"),axis.text=element_text(color="#668080"))+
theme(strip.text.x = element_text(color="#668080"))+
theme(legend.position = "none")+
ylab("Share of young people")+
xlab("")
Since the health behaviour and mental well-being of young people are related to their family’s economic situation, the following analysis has been adjusted to accommodate the effect of this connection. The following results were also adjusted for the home language in order to eliminate the influence of different cultural backgrounds on the occurrence of a depressiveness. Therefore, to gain a better understanding of lifestyle factors associated with mental well-being, the analysis took into account the family’s economic background, young people’s home language, and age, to eliminate the effect of variation caused by these characteristics. Figure 2.2.5 provides an overview of the relationship between experiencing periods of depressiveness and various lifestyle factors (diet, physical activity, body image, sleep patterns and smoking, alcohol and cannabis use) in girls and boys. The relationships described in the figure are not necessarily causal; that is, they could be in either direction.
For healthy development, the young body needs plenty of fruits and vegetables, unrefined grain products, and moderate amounts of protein-rich foods. It needs only minimal amounts of sugary and processed foods; though high in energy, these lack important micronutrients. In our analysis, we assessed the relationship between diet and mental well-being based on the frequency of vegetable and fruit consumption and the eating of breakfast, in relation to the occurrence of periods of depressiveness. The reason for selecting these nutrition-related characteristics is that eating sufficient amounts of vegetables and fruits has generally been associated with better health. Anywhere upwards from seven or eight portions of vegetables and fruits every day, which is approximately 700 to 800 grams, is considered a sufficient amount for adolescents. Eating breakfast regularly is also known to be associated with better general well-being, including a lower risk of being overweight (Szajewska and Ruszczyński 2010) and a more positive body image (Ramseyer et al. 2019).
Our analysis indicates that mental wellbeing is closely associated with nutrition. The adolescents who consumed fewer vegetables and fruits than recommended had 1.3−1.5 times the odds of depressiveness (Figure 2.2.5). Furthermore, both girls and boys who regularly skipped breakfast were twice as likely to experience periods of depressiveness as the adolescents who ate breakfast.
Besides nutrition, sedentary lifestyle and physical inactivity are the two key determining factors of adolescent lifestyle and health (Biddle et al. 2017). According to WHO recommendations, young people should spend an average of at least one hour a day engaging in moderate to intense physical activity. Based on Estonian data, 16% of young people meet the recommended levels of physical activity (Oja et al. 2019). Adolescents’ level of physical fitness is an important indicator of their lifestyle and has a positive correlation with quality of life. Furthermore, low physical activity is associated with risk factors for lifestyle-related diseases that may follow into adulthood.
The results of our analysis confirm the association between mental wellbeing and physical activity: Figure 2.2.5 shows that adolescents who were less physically active had up to 1.4 times the odds of depressiveness.
Diet and physical activity are often connected with excessive weight or the fear of being overweight, which in turn can affect a young person’s body image. A negative body image can lead to less healthy choices, such as extreme dieting or over-exercising. The rate of young people who had experienced periods of depressiveness and had suicidal thoughts within the previous 12 months was higher among adolescents who were overweight (Haav 2020). Seetõttu kuulub vaimse heaolu juurde positiivse kehakuvandi säilitamine. herefore, maintaining a positive body image is a part of mental well-being. According to Estonian data from 2018, slightly more than a third (34%) of school students considered themselves fat, girls more often than boys (38% v. 30%). A comparison with body mass index demonstrated that the body image of the majority of students was appropriate (Oja et al. 2019). Figure 2.2.5 shows that girls with a negative body image had more than double the odds of experiencing depressiveness, and while the odds are lower for boys, a negative body image was significantly associated with mental well-being among them as well.
An optimal sleep regime is another important part of a healthy lifestyle. Insufficient sleep in adolescents is a growing public health problem in many countries. Poor sleep patterns, including insufficient, inconsistent, interrupted or poorly timed sleep (e.g. late bedtimes), affect between 30% and 70% of young people in Europe. At least a quarter of young people have trouble falling asleep at night and feel tired during the day. Adolescents’ sleep patterns differ between schooldays and days off and do not meet their sleep requirements (Gariepy et al. 2020). The share of young people meeting the requirements for sleep duration is significantly lower on schooldays (from 32% to 86%) than it is on weekends (from 79% to 92%). The duration of sleep of Estonian adolescents also varies a great deal between schooldays and weekends. The scores are similar to the European average – 72% of Estonian adolescents meet the recommended duration of sleep on schooldays, while 92% meet the recommendation on weekends (Oja et al. 2019).
The effect of insufficient sleep on depressiveness was stronger among girls, who had more than double the odds of experiencing periods of depressiveness if they failed to get enough sleep (Figure 2.2.5). While the relation to sleep duration is slightly weaker in boys than in girls, it remains significant.
J2.2.5.R
maiko.koort
2023-06-27
library(ggplot2)
library(scales)
#faili sisselugemine ja andmete formaadi korrigeerimine
J225=read.csv2("PT2-T2.2-J2.2.5.csv",header=TRUE, encoding ="UTF-8")
J225$OR=as.numeric(J225$OR)
J225$CI.upper=as.numeric(J225$CI.upper)
J225$CI.lower=as.numeric(J225$CI.lower)
J225$Väärtus=as.factor(J225$Väärtus)
J225$Tunnus=as.factor(J225$Tunnus)
J225$Tunnus=factor(J225$Tunnus,levels(J225$Tunnus)[order(c(1,8,5,4,2,7,3,9,6))])
J225$Väärtus=factor(J225$Väärtus,levels(J225$Väärtus)[order(c(2,1,3,9,13,6,7,8,4,10,11,12,5))])
#joonis
ggplot(J225)+
geom_point(aes(x=Väärtus,y=OR,col=Sugu),cex=3)+
geom_errorbar(aes(x=Väärtus,ymin=CI.lower,ymax=CI.upper,col=Sugu),width=0.3, linewidth=0.8)+
geom_abline(aes(slope=0,intercept=1))+
scale_y_continuous(breaks=c(1,2,3,4,5,6,7,8))+
facet_grid(Tunnus~Sugu,scales="free_y")+
theme_light()+
theme(legend.position = "none")+
coord_flip()+
xlab("")+
ylab("")+
theme(strip.text.y = element_text(angle = 360,color="#668080"),strip.text.x=element_text(color="#668080"),strip.background =element_rect(fill="white"))+
scale_color_manual(values=c("#6666cc","#FF3600"))+
theme(text = element_text(color="#668080"),axis.text=element_text(color="#668080"))
Drugs included in the analysis are alcohol, cigarettes and cannabis. Recent studies have shown that the number of young people who have consumed alcohol during their lifetime has decreased somewhat, while the number of young people who drink alcohol frequently and regularly has not changed (Vorobjov and Tamson 2020). For example, 37% of 15-to-16-year-old adolescents report that they have consumed alcohol in the last month, and a third have been drunk at least once in their life. As a disturbing trend, strong alcohol makes up a large proportion of the alcoholic beverages consumed by adolescents, increasing the risk of alcohol poisoning. Although there were no differences in alcohol consumption and intoxication between girls and boys, our analysis showed that the experience of periods of depressiveness was twice as frequent among girls who have been drunk than among boys. Our analysis showed that girls who have been drunk twice or more in their life had more than three times the odds of depressiveness as those who have never been drunk (Figure 2.2.5).
The use of different drugs is interrelated. In most cases, young people first experiment with cigarettes and alcohol before moving on to other substances, most often cannabis or stimulants (Vorobjov and Tamson 2020). As with alcohol, the use of cannabis is strongly associated with depressiveness. Based on our analysis, girls and boys who have used cannabis had nearly four times the odds of experiencing periods of depressiveness.
Over the last two decades, cigarette smoking among adolescents has decreased significantly. Our analysis (Figure 2.2.5), showed that girls who smoked at least once a week experienced periods of depressiveness almost five times as frequently as their non-smoking peers. For boys it was over twice as frequently as their non-smoking peers.
Summary
While the quality of life of young people in Estonia has never been as good as it is now, their mental well-being and health and risk behaviour characteristics show negative trends. In addition to the health and risk behaviour and socioeconomic characteristics viewed in this article, young people’s lifestyle choices are influenced by their relationships with family, friends and people at school, which are discussed in the article by Valk et al. (‘Mental health and well-being in the learning environment’) in Chapter 3 of this report.
In the last decade, sadness, depressive symptoms and depressiveness have grown more frequent among young people in Estonia and neighbouring countries. While girls experience mental health problems more often, the prevalence of mental problems increases with age in girls and boys alike. Factors that support young people’s mental wellbeing include a healthy diet with adequate physical activity and sleep.
Indicators of poor mental health are strongly associated with drug use, whether that be cigarettes, alcohol or narcotics. Our results also indicate that young people living in a poor economic situation and speaking a language other than Estonian as their home language experience periods of depressiveness more frequently, which suggests social inequality and needs to be treated separately. Based on the results, we present recommendations below for encouraging young people to make constructive lifestyle choices.
Family and the example set by parents play an important role in shaping the nutrition habits of young people. Recommendations for promoting a healthier diet include making healthy food more appealing and increasing the accessibility and convenience of healthy choices while limiting unhealthy ones. It is also important to encourage healthy nutritional behaviour at an early age and to make health-conscious eating trendy through social norms.
In developing young people’s physical activity, physical education at school should focus more on supporting students’ independent physical activity and exercise habits outside of school. This could include instructions for independent practice on local exercise tracks or outdoor sports grounds, which could be used for physical activity with levels of difficulty and intensity appropriate for the school level. Teachers could follow students’ progress by asking them to document their path of movement or visit to the sports grounds by tracking their physical activity via screenshots from a smartwatch or phone app.
Poor sleep quality is associated not only with poorer mental health but also with more frequent risk behaviour in adolescents. It has been found that in addition to ensuring longer sleep duration, parents who have set a suitable bedtime for their school-aged children contribute to their greater daytime alertness and mental well-being (Peltz et al. 2020). his involves following sleep hygiene, which may include avoiding the use of electronic devices right before sleep or limiting the consumption of caffeinated beverages. The improved quality of sleep and higher well-being of young people has also been confirmed to be positively associated with a later start to the school day (Peltz et al. 2017). Some Estonian schools have moved towards starting classes at 9 am instead of 8 am or having one day a week when classes start much later, for example, at 10 am.
Substance use prevention is part of the personal, social and health education curricula at Estonian schools. Drug education must be broad-based and does not mean specifically discussing various drugs and their effects but involves the development of personal and social skills. These include communication skills, such as conflict management, self-awareness and saying no, as well as self-management skills to cope with stress, anxiety and other emotions. In addition to the curriculum, there are several prevention programmes launched by the National Institute for Health Development that are school-based (VEPA, KIVA), but also support parent education (Tark Vanem, Imelised aastad, EFEKT). All of these programmes aim to foster a safe and supportive environment for the development of young people. Data show that even minor drug use among lower secondary school students is associated with a higher risk of developing mental disorders (Brownlie et al. 2019). However, sometimes it is also the other way around: people may turn to drugs to cope with their mental health issues. Regardless of the situation, it is extremely important to recognise the problem as it emerges and intervene at an early stage.
Current research on prevention stresses the importance of a supportive environment to prevent risk behaviour in young people and to increase their mental wellbeing. (Hawkins et al 2015). Fostering a supportive environment for young people means dealing with both the psychosocial and physical environment. It means promoting the prosocial behaviour of young people, instilling values and imposing rules in both the home and school environments (Biglan et al. 2012). The psychological flexibility of parents/teachers and their willingness to cooperate are essential to a supportive environment. One of the forms of cooperation that supports the development of an adolescent is a mentor-mentee relationship with an adult, especially in circumstances where the support of the parent(s) is not viable or adequate. A mentor can be someone from the school staff, a coach or an adult leading extracurricular activities. The goal of the mentorship is to cultivate a positive self-image in the young person, thereby promoting their positive behaviour, including in matters of health.
To sum up, our findings show that a healthy lifestyle in young people is associated with better mental health and well-being; the adults who surround young people, and ensure a supportive and safe environment, play a vital role in setting the factors that affect the health behaviour of young people.
Biddle, S. J., García Bengoechea, E., & Wiesner, G. (2017). Sedentary behaviour and adiposity in youth: a systematic review of reviews and analysis of causality. International Journal of Behavioral Nutrition and Physical Activity, 14(1), 1–21.
Biglan, A., Flay, B. R., Embry, D. D., & Sandler, I. N. (2012). The critical role of nurturing environments for promoting human well-being. American Psychologist, 67(4), 257.
Brownlie, E., Beitchman, J. H., Chaim, G., Wolfe, D. A., Rush, B., & Henderson, J. (2019). Early adolescent substance use and mental health problems and service utilisation in a school-based sample. The Canadian Journal of Psychiatry, 64(2), 116–125.
Gariepy, G., Danna, S., Gobiņa, I., Rasmussen, M., de Matos, M. G., Tynjälä, J., … & Schnohr, C. (2020). How are adolescents sleeping? Adolescent sleep patterns and sociodemographic differences in 24 European and North American countries. Journal of Adolescent Health, 66(6), S81–S88.
Haav, A. (2020). Noorte ülekaalulisus ja sellega seotud tegurid. Eesti Arst, 99 (Lisa 1), 24−31.
Hawkins, J. D., Jenson, J. M., Catalano, R., Fraser, M. W., Botvin, G. J., Shapiro, V., … & Stone, S. (2016). Unleashing the power of prevention. American Journal of Medical Research, 3(1), 39.
Inchley, J. C., Stevens, G. W., Samdal, O., & Currie, D. B. (2020). Enhancing understanding of adolescent health and well-being: The health behaviour in school-aged children study. Journal of Adolescent Health, 66(6), S3–S5.
Kessler, R. C., Angermeyer, M., Anthony, J. C., De Graaf, R. O. N., Demyttenaere, K., Gasquet, I., … & Üstün, T. B. (2007). Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World psychiatry, 6(3), 168–176.
Moore, S. A., Dowdy, E., Nylund-Gibson, K., & Furlong, M. J. (2019). A latent transition analysis of the longitudinal stability of dual-factor mental health in adolescence. Journal of School Psychology, 73, 56–73.
Oja, L., Piksööt, J., Aasvee, K., Haav, A., Kasvandik, L., Kukk, M., Kukke, K., Rahno, J., Saapar, M., Vorobjov, S. (2019). Eesti kooliõpilaste tervisekäitumine. 2017/2018. õppeaasta uuringu raport. Tallinn: Tervise Arengu Instituut, alla laaditud 25.09.2022 https://tai.ee/et/valjaanded/eesti-kooliopilaste-tervisekaitumine-20172018-oppeaasta-uuringu-raport
Peltz, J. S., Rogge, R. D., Connolly, H., & O’Connor, T. G. (2017). A process-oriented model linking adolescents’ sleep hygiene and psychological functioning: the moderating role of school start times. Sleep Health, 3(6), 465–471.
Peltz, J. S., Rogge, R. D., & Connolly, H. (2020). Parents still matter: the influence of parental enforcement of bedtime on adolescents’ depressive symptoms. Sleep, 43(5), zsz287.
Ramseyer Winter, V., Jones, A., & O’Neill, E. (2019). Eating breakfast and family meals in adolescence: the role of body image. Social Work in Public Health, 34(3), 230–238.
Szajewska, H., & Ruszczyński, M. (2010). Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in Europe. Critical Reviews in Food Science and Nutrition, 50(2), 113–119.
Vorobjov. S., & Tamson, M. (2020). Uimastite tarvitamine koolinoorte seas: tubakatoodete, alkoholi ja narkootiliste ainete tarvitamine Eesti 15–16-aastaste õpilaste seas. Tallinn: Tervise Arengu Instituut, alla laaditud 25.09.2022 https://tai.ee/sites/default/files/2021-03/159103814529_Uimastite_tarvitamine_koolinoorte_seas_2019.pdf